Diversifying Georgia’s Health Workforce Could Expand Access, Improve Care
As the population of Georgia continues to rapidly grow and diversify, it is important that the health care system keeps up to serve more patients from a wide range of racial and ethnic backgrounds. Training and attracting new providers is critical to meet the state’s health care needs. But a strong health care workforce should also reflect the growing diversity of Georgia communities.
A diverse health care workforce is associated with improving access to care in racial and ethnic minority communities, ensuring greater patient choice and satisfaction and improving the quality of health care for vulnerable people. Working to build a more equitable and diverse health care workforce could bring three key benefits to all Georgians.[1]
Better access to care for underserved communities. Minority health care providers are more likely to practice in underserved communities and more likely to enter primary care specialties than their white counterparts. The shortage of primary care providers and overall scarcity in underserved rural areas is an urgent problem in Georgia. Recruiting a more diverse workforce can help remove barriers to health care access in the state’s medically-underserved areas.
Higher quality of care for vulnerable populations. Patient choice and satisfaction are greatly improved when minorities are well-represented in the health care workforce. Improving quality of care for the most vulnerable groups can improve the state’s overall health outcomes, which in turn can cut health care system costs over the long run.
Access to more culturally competent care. Georgia needs culturally competent health professionals to provide better care to an increasingly diverse population. Diversity in health professional programs and provider teams is proven to lead to more cultural competence among all health care providers.
To unlock the benefits of a more diverse health workforce, Georgia needs to attract more minorities and continue to retain and attract foreign-born health professionals who are already filling key gaps in the state’s health care network. Potential solutions include:
- Scholarships, loan repayment and other financial incentives to remove financial barriers for minorities and rural residents seeking health professional careers
- Increased support for pipeline training programs and diversity initiatives at health professional schools
- Required cultural competency training for health care providers
- Inclusive immigration policies to establish a welcoming environment for foreign-born health professionals
Georgia’s Health Workforce Trails Demographic Changes
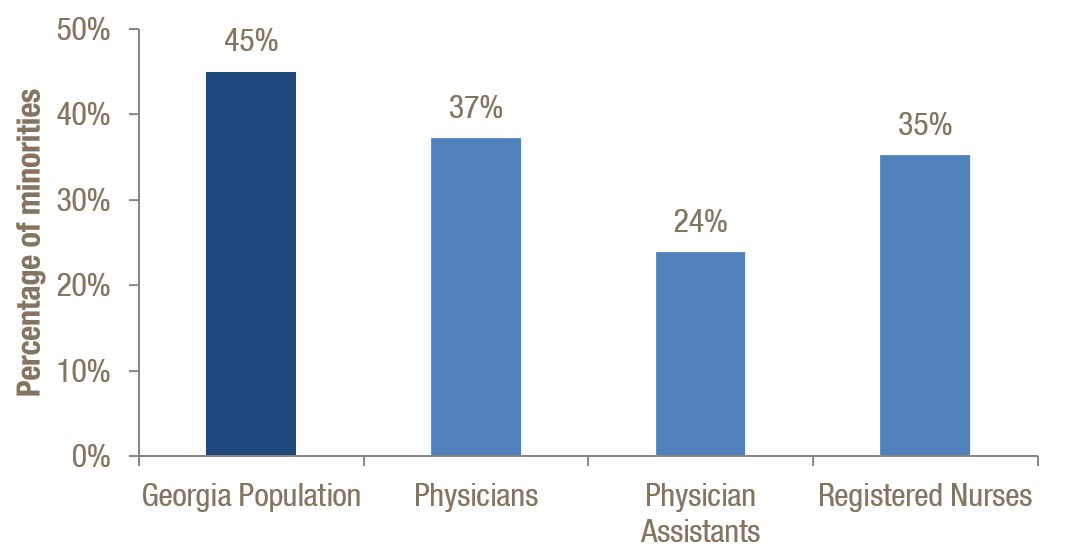
By the year 2044, more than half of the United States population is projected to belong to a racial or ethnic minority group.[2] Georgia is close to this majority-minority threshold with 45 percent of Georgians belonging to a racial or ethnic minority group in 2014, the most recent year available.[3] This analysis counts minorities as all non-white populations, including people who identify as black, non-white Hispanic, Asian, Native American, Native Hawaiian and Pacific Islander or other.
Georgia’s population in 2014 was 55 percent white, 30 percent black, 9 percent Hispanic, 4 percent Asian and 2 percent from other groups. This is an increase of 8 percentage points from 2000 when racial and ethnic minorities accounted for 37 percent of Georgia’s population.[4] Hispanics accounted for the largest increase, growing from 5 percent of the population in 2000 to 9 percent in 2014. The Asian population in Georgia increased from 2 percent to 4 percent from 2000 to 2014, and the black population increased from 29 percent to 30 percent.
Although minorities make up about 45 percent of Georgia’s population, they are underrepresented among frontline medical providers. Georgia’s minorities account for only 24 percent of physician assistants, 35 percent of registered nurses and 37 percent of physicians.
Minorities are Underrepresented in Georgia’s Healthcare Workforce
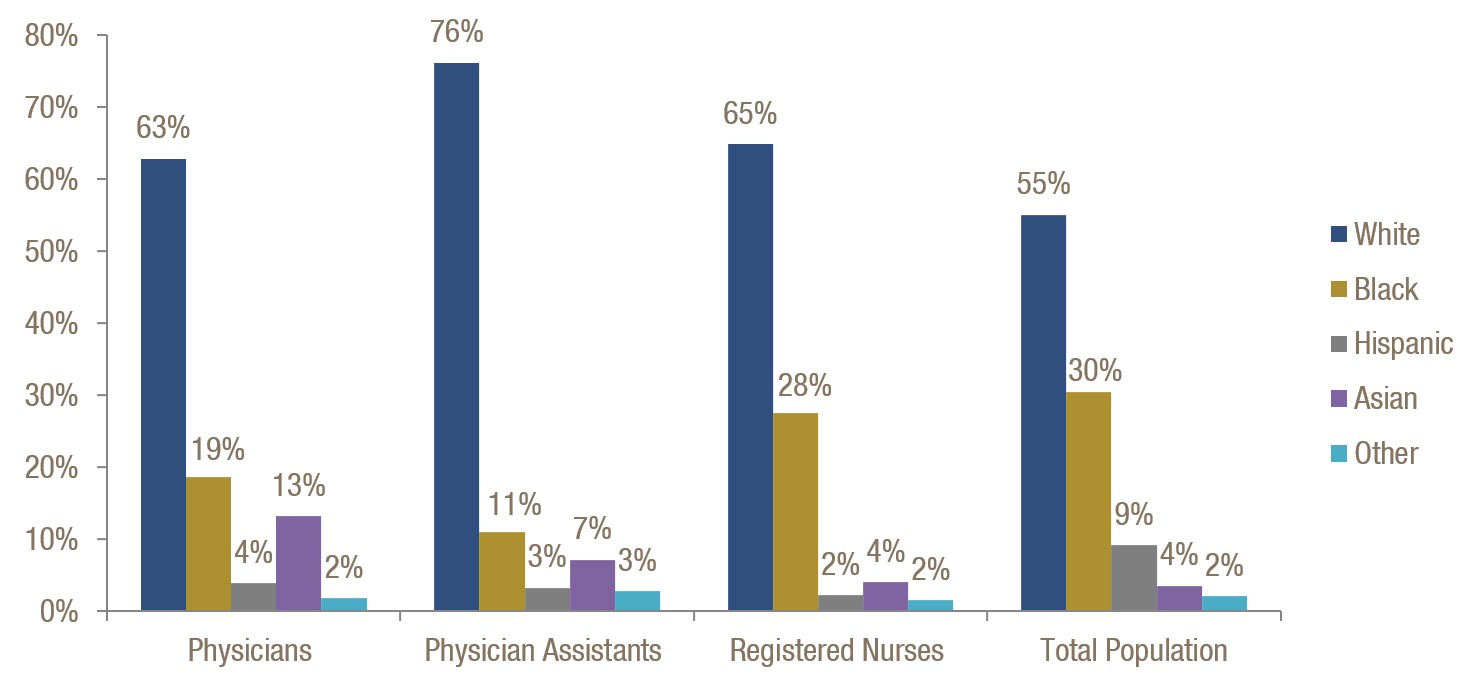
While minorities are underrepresented among health care providers overall, the variation among groups and provider types is considerable. Asian physicians account for a significantly higher share than in the general population[*], while the opposite is true for black and Hispanic doctors. Black people are well represented among Georgia nurses, while Hispanics are not. Understanding where the shortages are can guide efforts to increase diversity among different types of health providers.
Minority Representation Varies Among Health Provider Types
Georgia Health Professionals by Race or Ethnicity
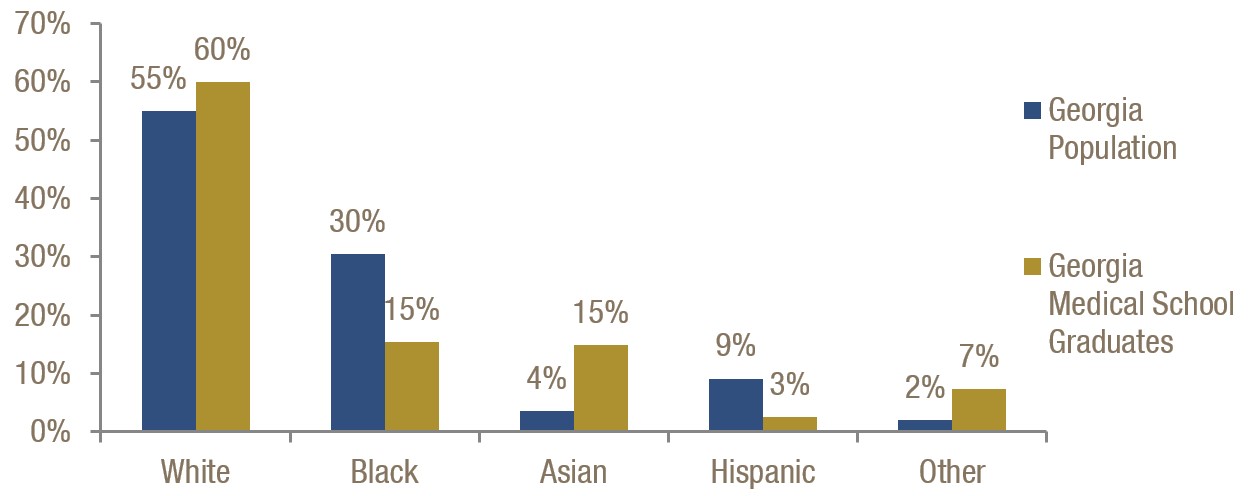
Graduates of Georgia’s medical schools better reflect the growing diversity of the state, with about 40 percent of them counted as racial and ethnic minorities.[5] Still, some racial and ethnic groups are underrepresented in Georgia medical school graduating classes. Thirty percent of Georgians are black, but only 15 percent of medical school graduates are. Hispanic Georgians make up 9 percent of the population but just 3 percent of the state’s medical school graduates. The overall growth in the share of medical school graduates who are minorities suggests Georgia can make strong progress toward a more diverse health care workforce by enticing more of these graduates to practice in the state.
Georgia Medical Schools Are Increasing Minority Enrollment, Better Reflecting the State’s Diversity
Medical School Graduates by Race or Ethnicity
Immigrants to Georgia Help Fill Key Provider Gaps
Some diversity gains in Georgia are due to the growth of the immigrant community, which is infusing the health care workforce with nurses and doctors. Ten percent of Georgians are foreign-born, a population that accounts for 10 percent of nurses and medical assistants and 23 percent of doctors.[6] The foreign-born population’s influence on the health care workforce is also evidenced by the large share of physicians and physician assistants who are Asian. Sixty-nine percent of Asian residents in Georgia are foreign born.[7]
The significant share of foreign-born doctors in the state boosts the number of health care providers and helps reduce cultural and language barriers. About 13 percent of Georgians speak a language other than English at home and 6 percent speak English less than very well. Lack of health care providers who can communicate with patients who speak limited to no English reduces health care access and quality of care. Since 28 percent of Georgia physicians say they speak a language other than English, some of the communication gap is mitigated.[8]
Georgia Stands to Gain from More Diverse Health Workforce
The evidence from other states and a wide range of academic studies is clear that Georgia can reap benefits from a more diverse health care workforce.[9] These benefits include:
- Increased access to care for underserved communities
- Higher quality of care for Georgia’s most vulnerable people
- More culturally competent care
Access to Care
Diversity in a health care workforce is invaluable to offering greater access to underserved people.[10] Minority doctors are much more likely to practice in underserved communities than white doctors.[11] Black and Hispanic physicians are more likely to care for low-income and Medicaid patients.[12] This also holds true for minority dentists and psychologists, who are more likely to practice in minority communities than their white peers.[13]
Georgia’s struggling rural hospitals treat a large proportion of patients with low incomes and insufficient insurance coverage to pay for services.[14] More than 1.4 million Georgians are uninsured.[15] Black and Hispanic Georgians make up 57 percent of the uninsured population despite accounting for about 39 percent of the state overall. Minorities are more likely to be uninsured and live in medically underserved areas. A diverse health care workforce can improve access to care and strengthen hospital treatment capacity in rural and underserved areas.
Many more minority physicians choose primary care specialties compared to white physicians.[16] Georgia’s health care worker shortage is most severe in primary care specialties.[17] Projections show to maintain current service levels Georgia needs 2,099 primary care physicians by 2030, a 38 percent increase from 2010.[18] The primary care workforce is not growing quickly enough, based on past trends. Georgia added 15 percent more primary care physicians from 2000 to 2010, while adding 37 percent more specialist physicians.[19] Recruiting and retaining minority physicians holds the potential to address overall shortages in primary care.
Quality of Care
A diverse health care workforce provides high-quality care to underserved communities.[20] Quality of care includes measures of patient choice and satisfaction. Those are greatly improved for minority patients when minorities are well represented in the health care workforce. Minority patients tend to rate their quality of care and satisfaction higher when they receive care from minority health professionals.[21] Unconscious bias develops early on in life, with children as young as three to five years old showing more favorable attitudes toward white people than people of other races. The same bias is found in studies with physicians and it can lead to differences in treatment and contribute to health disparities.[22] One example of unconscious bias is that black and Hispanic patients are less likely to receive appropriate cardiac medication than other racial and ethnic groups, even taking into account insurance status, income, age and symptoms. [23] Black and Hispanic patients are more likely to follow medication instructions after they get treatment from someone of the same racial or ethnic background.[24]
Vulnerable groups can get significantly better results from better quality of care. Georgia ranked 46th in overall health in 2015 out of 50 states and the District of Columbia.[25] The state ranks better in areas such as avoidable hospital use and costs, but poorly in access and equity. One in five Georgia adults reported going without care in the past year due to cost.[26] The state also ranked 45th by health equity measures. Hispanic residents in Georgia are more likely to lack a usual source of health care. Fifty-six percent of Georgia’s Hispanics say they lack a usual source of care, compared to 30 percent of black people and less than 25 percent of white people.[27]
56%
Share of Hispanics in Georgia without a usual source of care – compared to 24% of Whites
Georgia can improve these measures and reduce the financial burden on its health care system when healthier patients need less care. Lost productivity and absenteeism are consequences when workers are ill, which weakens the overall economy. The business community already recognizes that a diverse workforce makes for a stronger economy. Businesses know a diverse workforce helps maintain competitiveness in the global marketplace and equips them with the skills to work and build consensus with people from different backgrounds and cultures. A more diverse health care workforce can generate significant savings in the long-term for state health costs as the minority population grows healthier. Residents not able to work or meet basic living expenses due to illness, high medical bills or lack of access to care are more productive after they get healthy.
46th
Georgia’s ranking in overall health among the 50 states and District of Columbia45th
Georgia’s ranking in health equity measures among the 50 states and District of Columbia
Cultural Competency
A diverse workforce can improve cultural competency among providers, which is a necessity in Georgia as the foreign-born population grows. Patients unfamiliar with western cultural norms in health and health care can hold views on health that change their treatment experience and results. Western values of individualism and dependence on technology can collide with values of collectivism and spirituality. Some Native American communities would benefit from an inclusion of alternative healing methods in their treatment plans. Respect and a personal connection are valued in many Hispanic cultures. Sensitively addressing older patients and getting to know them and their families can be a more effective approach to caring for them.[28] More health care providers with personal exposure to minority and ethnic cultural beliefs can improve the quality of care and resulting health for patients from a range of cultural backgrounds.
Culturally competent health care professionals offer the awareness, knowledge and skills needed to provide care for patients from a range of backgrounds.[29] Cultural competency is most effectively gained through training in an educational setting that allows students to interact with people from different racial and ethnic backgrounds and nationalities.[30] Diversity in health professional schools and health provider teams not only benefits minority communities but effectively trains all providers to become more culturally competent.[31]
Georgia Lawmakers Can Help Build More Diverse Health Workforce
State policymakers already recognize the urgent need for more providers to improve access to care in underserved rural areas. Training and attracting more minorities is a proven way to build workforce capacity in the areas with the greatest need. Attracting and retaining foreign-born health professionals is also part of this strategy.
Georgia residents agree a diverse health care workforce is important. Seventy-two percent of Georgians in a statewide poll said they believe it is important to have enough black and Hispanic health professionals to reflect the population they serve.[32] Georgia schools are making efforts to train more minority doctors. [33] The historically black Morehouse School of Medicine graduates the most primary care health professionals in Georgia.[34] Morehouse also encourages students to practice in rural areas, requiring students to conduct some of their clinical rotation obligations in a rural community.[35]
With this robust interest in a stronger and more diverse workforce and a health care system straining to keep up with the need, now is time for state policymakers to take action. Here are some strategies.
Scholarships and Loan Repayment
The wealth gap between the white population and minority groups is profound. Minorities, especially black and Hispanic groups, are overrepresented in poverty. Financial barriers to health professional training are disproportionately high for minority students. Scholarships, tuition reimbursement and loan forgiveness opportunities are important tools to recruit these students. The state now offers a loan forgiveness program for physicians practicing in rural areas, but the investment is small compared to the growing need. Georgia can improve health care capacity and attract minority professionals by expanding this program. Lawmakers can also create new financial incentives for doctors and other health professions, such as expanding a modest tax credit already available for doctors who serve in rural areas.[36]
Education and Training Programs
Only half of Georgia medical school graduates stay in the state to practice. If the student completed a residency program in the state, that increases to 70 percent.[37] Programs such as Pathway to Med School in southwest Georgia are working to encourage in-state students to remain to practice after their training. That program prioritizes recruitment of college students from rural Georgia counties and 87 percent of students in its last 12 graduating classes who applied for medical school were admitted.[38] Expansion of these successful pipeline programs for Georgia students from rural areas and/or racial and ethnic minorities can increase the likelihood of rural and minority health care providers continuing to practice in these areas.
50%
Share of Georgia medical school graduates who practice in-state70%
Share of Georgia medical school graduates who practice in-state if student completed a Georgia residency program
More residency program slots to accommodate additional Georgia medical school graduates can also help retain the increased diversity medical schools established over the years. Georgia ranks 40th among the states in the number of medical residents per 100,000 people and needs to add about 465 residency slots to reach the national average.[39] Georgia policymakers can continue to support the work medical schools are doing to increase diversity by guiding the accreditation and curriculum review process to ensure institutions meet national standards.[40]
University and health professional schools are just part of the remedy. Policymakers can provide adequate funding for quality K-12 education in minority communities, which often face unequal educational opportunity. Two-year colleges can also play an important role preparing students for allied health professions or to later attend health professional schools.[41]
Training Requirements
Indiana, Massachusetts, Missouri, Ohio, Oklahoma and Washington introduced legislation requiring health care professionals to acquire cultural competency training.[42] These bills required health care professionals seeking licensure to complete cultural competency instruction in school and/or through continuing education.
Inclusive Immigration Policies
Georgia can attract and retain foreign-born professionals by implementing policies to create a welcoming environment for foreign-born workers. These policies can include targeted efforts such as English language training for adults and children and programs to support immigrant entrepreneurs. The state’s lack of a tuition equity policy that allows young immigrant residents to pay in-state tuition is one area holding the state back from being an inclusive environment that supports a diverse workforce.
Conclusion
Georgia can build a diverse workforce to better serve residents in need of care and improve health throughout the state. The state is facing severe health care provider shortages. More than two-thirds of Georgia counties fall below the statewide average of nurses, doctors, physician assistants and primary care doctors per 100,000 residents. A rural hospital crisis in Georgia is evidenced by at least nine hospitals closing since 2001. More hospitals still struggle to cover uncompensated care costs and attract health care providers. Georgia must ensure it attracts not just more health care providers, but also the right mix. A diverse workforce can help achieve this goal by attracting minority health professionals who are more likely to enter primary care and work in underserved rural areas.
Georgia’s overall economy stands to benefit from the health improvements that a diverse health workforce would bring for vulnerable people. When people get healthier, they are able to be more productive workers and contribute to the economy at their full potential.
The high representation of the Asian and foreign-born community in Georgia’s health professions shows that greater diversity is already helping increase treatment capacity. Fixing the underrepresentation of black and Hispanic health professionals will benefit Georgia’s health care system even more.
Endnotes
[*] The different ethnicities within the Asian population (e.g. Vietnamese, Chinese, Indian, Korean, Filipino, Thai, etc.) are not all equally represented in health professions. Hmong, Laotian, Cambodian, and Malaysian groups are among those underrepresented nationally. There is a need for more data to understand provider capacity in different Asian communities.
[1] Smedley BD, Butler AS, Bristow LR (2004). In the Nation’s Compelling Interest: Ensuring Diversity in the Health-Care Workforce. Washington, DC: Institute of Medicine.
[2] U.S. Census. Projections of the Size and Composition of the U.S. Population: 2014 to 2060.
[3] American Community Survey 2014 Estimates
[4] 2010 Census and 2000 Census
[5] Kaiser Family Foundation (2015). Distribution of Medical School Graduates by Race/Ethnicity. http://kff.org/other/state-indicator/distribution-by-race-ethnicity/#
[6] Tharpe W (2015). Immigrants Help Chart Georgia’s Course to Prosperity. Georgia Budget and Policy Institute.
[7] American Community Survey 2014 Estimates
[8] Georgia Board for Physician Workforce. Georgia Physician and Physician Assistant Professions Data Book 2010/2011. http://gbpw.georgia.gov/gbpw-data-book
[9] Smedley BD, Butler AS, Bristow LR (2004). In the Nation’s Compelling Interest: Ensuring Diversity in the Health-Care Workforce. Washington, DC: Institute of Medicine.
[10] Smedley BD, Butler AS, Bristow LR (2004). In the Nation’s Compelling Interest: Ensuring Diversity in the Health-Care Workforce. Institute of Medicine.; Kington R, Tisnado D, Carlisle DM (2001). The Right Thing to Do, The Smart Thing to Do: Enhancing Diversity in the Health Professions. National Academy Press; Cohen JJ, Gabriel BA, Terrell C (2002). The Case For Diversity In The Health Care Workforce. Health Affairs.; U.S. Department of Health and Human Services (2011). HHS Action Plan to Reduce Racial and Ethnic Health Disparities: A Nation Free of Disparities in Health and Health Care.
[11] Kington R, Tisnado D, Carlisle DM (2001). The Right Thing to Do, The Smart Thing to Do: Enhancing Diversity in the Health Professions. National Academy Press; Smedley BD, Butler AS, Bristow LR (2004). In the Nation’s Compelling Interest: Ensuring Diversity in the Health-Care Workforce. Institute of Medicine.
[12] Cohen JJ, Gabriel BA, Terrell C (2002). The Case For Diversity In The Health Care Workforce. Health Affairs.; Cantor JC, Miles EL, Baker LC, Barker DC (1996). Physician Service to the Underserved: Implications for Affirmative Action in Medical Education. Inquiry.
[13] Smedley BD, Butler AS, Bristow LR (2004). In the Nation’s Compelling Interest: Ensuring Diversity in the Health-Care Workforce. Washington, DC: Institute of Medicine.
[14] Atlanta Journal-Constitution (2016). Georgia’s rural hospitals: trying to stay open. http://investigations.blog.ajc.com/2016/01/25/georgias-rural-hospitals-trying-to-stay-open/
[15] Kaiser Family Foundation (2015). Health Insurance Coverage of the Total Population. http://kff.org/other/state-indicator/total-population/
[16] Kington R, Tisnado D, Carlisle DM (2001). The Right Thing to Do, The Smart Thing to Do: Enhancing Diversity in the Health Professions. National Academy Press.
[17] Georgia Health News. Doctor shortage remains acute in rural areas.http://www.georgiahealthnews.com/2014/01/doctor-shortage-acute-rural-areas/
[18] Petterson SM; Cai A; Moore M; Bazemore A. State-level projections of primary care workforce, 2010-2030. September 2013, Robert Graham Center, Washington, D.C.
[19] Georgia Board for Physician Workforce. Georgia Physician and Physician Assistant Professions Data Book 2010/2011. http://gbpw.georgia.gov/gbpw-data-book
[20] Cohen JJ, Gabriel BA, Terrell C (2002). The Case For Diversity In The Health Care Workforce. Health Affairs.
[21] Smedley BD, Butler AS, Bristow LR (2004). In the Nation’s Compelling Interest: Ensuring Diversity in the Health-Care Workforce. Washington, DC: Institute of Medicine.
[22] The Joint Commission (2016). Implicit bias in health care. QuickSafety. Issue 23. https://www.jointcommission.org/assets/1/23/Quick_Safety_Issue_23_Apr_2016.pdf
[23] Smedley B, Stith A, Nelson A (2003). Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Institute of Medicine.
[24] Agency for Healthcare Research and Quality (2013). Quality of Care/Patient Safety. http://www.ahrq.gov/research/findings/factsheets/minority/minorfind/minorfind4.html
[25] McCarthy D, Radley DC, and Hayes SL (2015). Aiming Higher: Results from a Scorecard on State Health System Performance, 2015 Edition, The Commonwealth Fund. http://datacenter.commonwealthfund.org/scorecard/state/12/georgia/
[26] McCarthy D, Radley DC, and Hayes SL (2015). Aiming Higher: Results from a Scorecard on State Health System Performance, 2015 Edition, The Commonwealth Fund. http://datacenter.commonwealthfund.org/scorecard/state/12/georgia/
[27] Kaiser Family Foundation (2014). The Georgia Health Care Landscape. http://kff.org/health-reform/fact-sheet/the-georgia-health-care-landscape/
[28] Juckett G (2013). Caring for Latino Patients. American Family Physician. http://www.aafp.org/afp/2013/0101/p48.html
[29] Campinha-Bacote J (2003). Many Faces: Addressing Diversity in Health Care. Online Journal of Issues in Nursing. Vol. 8 No. 1. Manuscript 2.
[30] Cohen JJ, Gabriel BA, Terrell C (2002). The Case For Diversity In The Health Care Workforce. Health Affairs.
[31] Smedley BD, Butler AS, Bristow LR (2004). In the Nation’s Compelling Interest: Ensuring Diversity in the Health-Care Workforce. Washington, DC: Institute of Medicine.
[32] Katz M, Bradshaw D, Nelson G (2009). Achieving Greater Health Equity: Georgians Support Workforce Diversity. Healthcare Georgia Foundation: HealthVoices Issue 1. http://www.healthcaregeorgia.org/uploads/file/HGF_HV_09_01_F.pdf
[33] Georgia Health News. Training minority doctors a big priority for Georgia. http://www.georgiahealthnews.com/2011/03/training-minority-doctors-huge-priority-georgia/
[34] Georgia Board for Physician Workforce (2012). Fact Sheet on Georgia’s Medical Schools.
[35] Georgia Health News. Training minority doctors a big priority for Georgia. http://www.georgiahealthnews.com/2011/03/training-minority-doctors-huge-priority-georgia/
[36] Regulation 560-7-8-.20 Rural Physician Credit. http://dor.georgia.gov/listing-rural-counties-purposes-rural-physician-credit
[37] Beitsch R (2015). To Address Doctor Shortages, Some States Focus on Residencies. http://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2015/08/11/to-address-doctor-shortages-some-states-focus-on-residencies
[38] Southwest Georgia Area Health Education Center. Pathway to Med School. http://www.sowega-ahec.org/pathway
[39] Bentley A (2016). Gaps in Care. Georgia Trend. http://www.georgiatrend.com/May-2016/Gaps-in-Care/
[40] National Conference of State Legislatures (2014). Diversity in the Healthcare Workforce. http://www.ncsl.org/documents/health/Workforcediversity814.pdf
[41] Sullivan LW (2004). Missing Persons: Minorities in the Health Professions, A Report of the Sullivan Commission on Diversity in the Healthcare Workforce.
[42] Fantacone J (2014). Looking to the Future: Improving the Diversity of the Health Care Workforce. http://altarum.org/health-policy-blog/looking-to-the-future-improving-the-diversity-of-the-health-care-workforce






