The American Health Care Act (AHCA) proposes substantial cuts to Medicaid and changes in the insurance marketplace sure to jeopardize health care coverage for hundreds of thousands of Georgians, hammer hospitals statewide and shift significant costs to the state. The proposed upending of the federal health law passed the U.S. House of Representatives on May 4, 2017. The U.S. Senate is working on its own version of the AHCA that would also repeal major provisions of the Affordable Care Act of 2010.The American Health Care Act contains five serious threats to Georgia’s well-being:
Deep cuts to Medicaid through a cap on federal funding would imperil at-risk Georgians and threaten hospitals’ bottom line. Nearly 2 million Georgia children, seniors, veterans and people with disabilities receive critical health coverage through the Medicaid program. Upending the federal health law threatens the care of these vulnerable Georgians by cutting federal Medicaid funding in Georgia by $4 billion over 10 years.[1] The bill fundamentally restructures Medicaid by capping federal funding based on past per-enrollee costs. A capped Medicaid structure puts Georgia at a disadvantage because it ranks 45th among states in Medicaid spending per enrollee. Locking in that historically low spending for the long haul promises to strain the state’s budget and require Georgia lawmakers to struggle with difficult decisions about cuts to Medicaid eligibility and benefits.
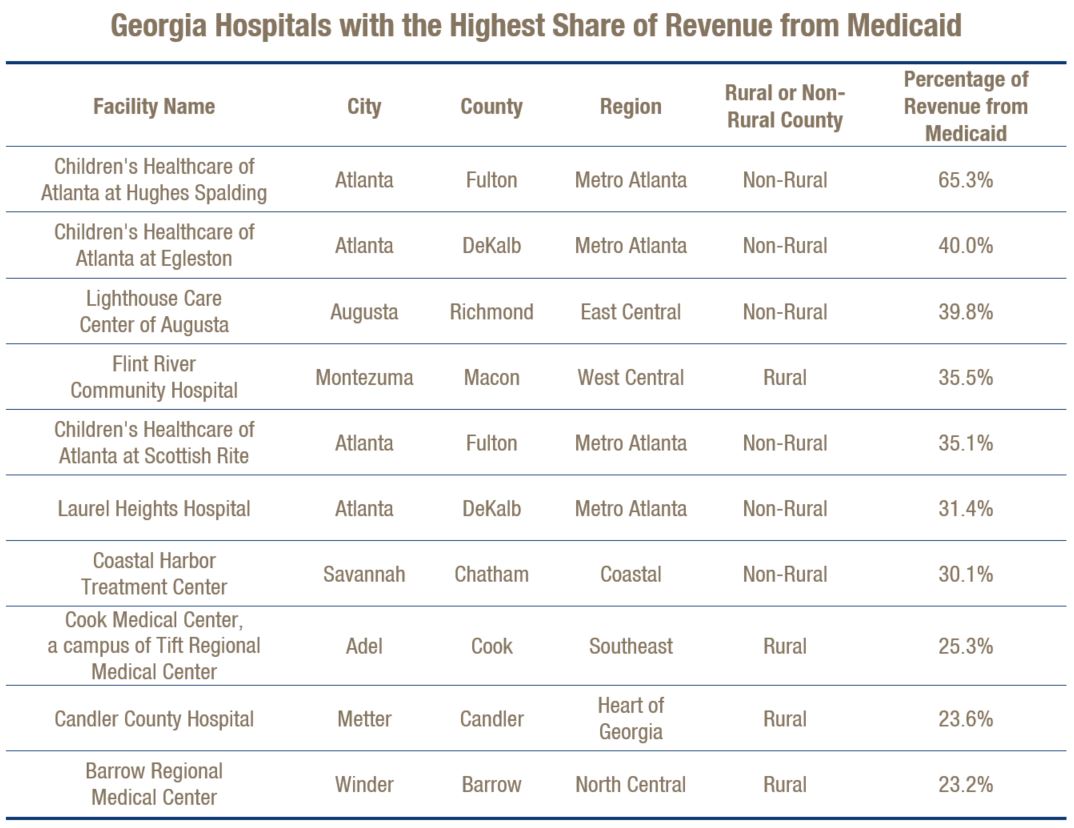
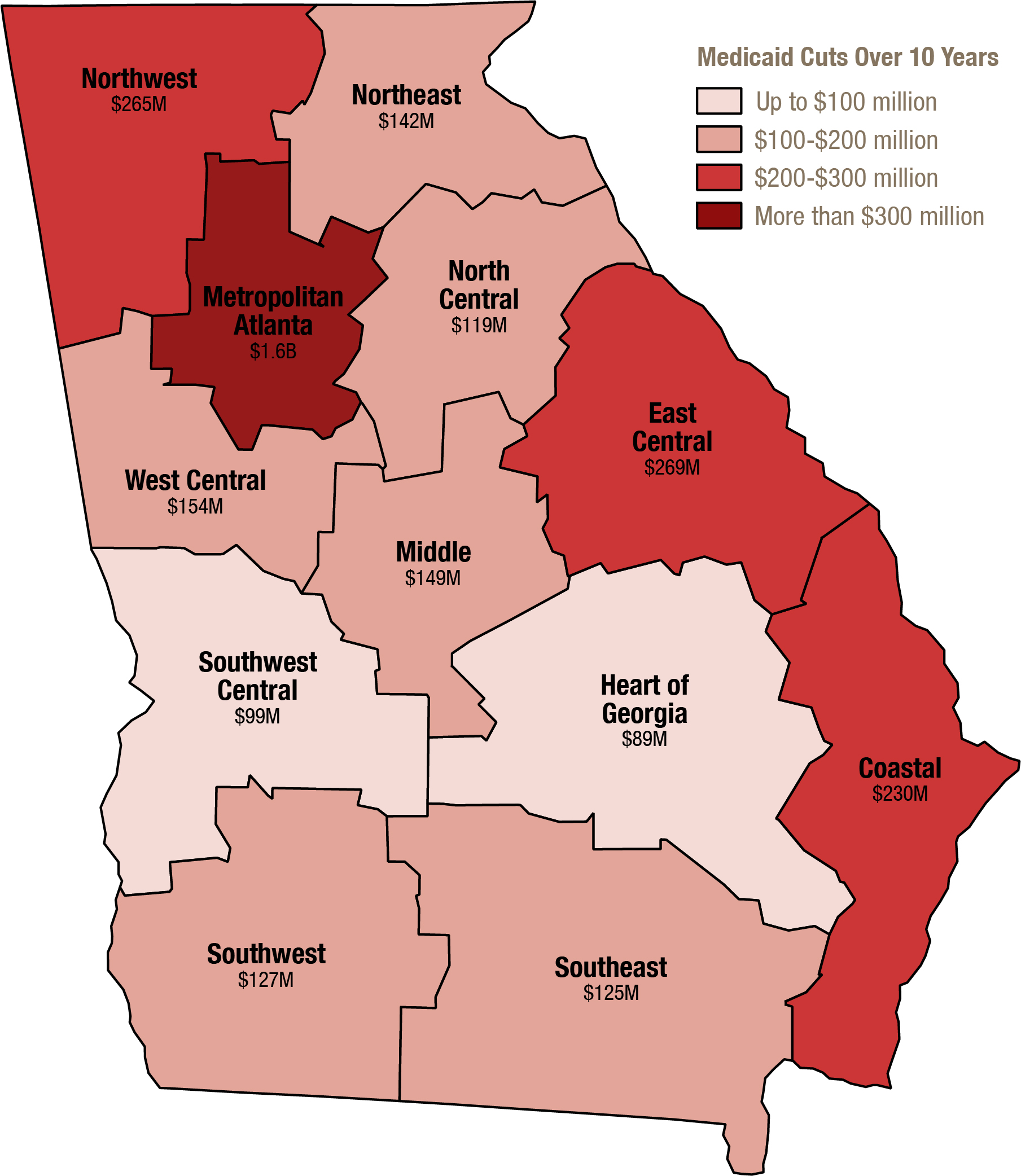
Any loss of Medicaid money poses special concern for Georgia’s hospitals. Hospitals in Georgia stand to lose an estimated $3.4 billion of Georgia’s $4 billion in total Medicaid cuts over the next 10 years. Communities in regions across the state are at risk, as opposed to just one or two large cities. Some of the estimated potential losses in the state’s health service delivery regions include $149 million in Middle Georgia, $127 million in Southwest Georgia, $265 in Northwest Georgia, $230 million in Coastal Georgia and $1.6 billion in metro Atlanta. Some of Georgia’s hospitals most at-risk from Medicaid cuts are Children’s Healthcare of Atlanta, Cook Medical Center in Adel and Lighthouse Care Center of Augusta.
Modifications to insurance subsidies will make it harder for Georgians to afford premiums, especially seniors and people in rural areas. The health insurance marketplace created by the Affordable Care Act enrolled almost half a million Georgians in 2017. The resulting coverage gains in Georgia prompted the uninsured rate among employed Georgians to fall by 22 percent from 2013 to 2015.[2] About 87 percent of Georgians who buy insurance in the marketplace can afford health coverage because they qualify for subsidies. The AHCA proposes to reduce subsidy amounts for many Georgians, causing many to lose coverage because they cannot afford insurance without the assistance.
The harmful effects of cuts to Medicaid and marketplace subsidies extend beyond the health care sector. Georgia school districts would also face a greater financial strain under the AHCA. Georgia schools received $30 million in Medicaid dollars in 2015 to provide services for special education students and pay school nurses and therapists to provide treatment and screenings for all children. With less funding flowing to the state through Medicaid and marketplace subsidies, Georgia’s economic outlook suffers. Georgia’s is projected to lose 16,200 jobs by 2026.
Giving states the option to water down consumer protections could reverse big gains for Georgians with pre-existing conditions or costly long-term health needs. Many Georgians with employer-based private insurance also benefited from the Affordable Care Act’s ban on denying coverage for pre-existing conditions and ban on setting annual and lifetime limits. Nearly 1.8 million Georgians carry a pre-existing condition that insurers used to deny coverage before the 2010 federal health law.[3] And 3.3 million Georgians no longer have lifetime limits on their plans because of the law. The AHCA gives states the option to change these regulations, allowing insurance companies to charge people with pre-existing conditions higher premiums or cover less of the benefits they need.
Axing the Prevention and Public Health fund eliminates a critical pool of money for state initiatives to keep Georgians healthy. The Affordable Care Act’s Prevention and Public Health Fund is repealed in the AHCA. Georgia stands to lose $20 million a year in public health funding over five years if the fund is lost. This funding is critical effectively respond to epidemics, reduce infant and maternal mortality, and prevent chronic disease among other efforts to improve Georgia’s relatively low health status.
Capping Medicaid Funding Leaves Georgia at a Disadvantage
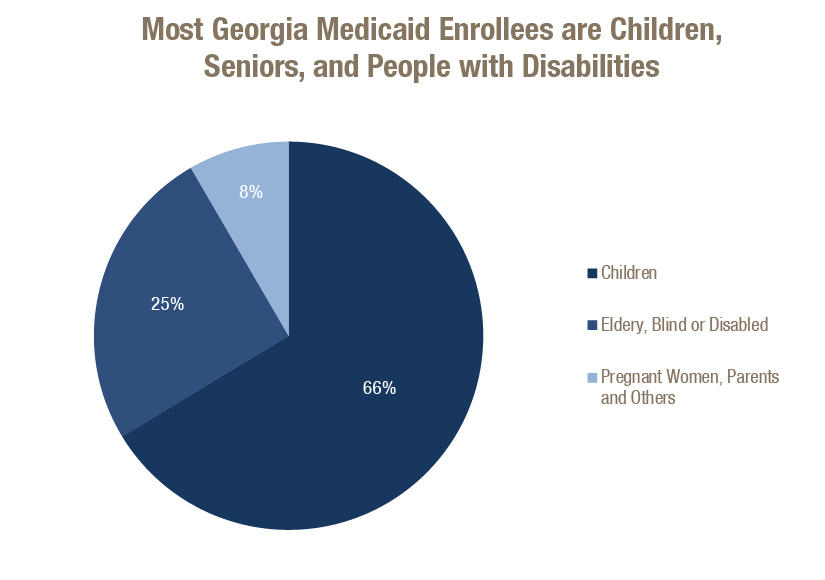
President Lyndon B. Johnson signed Medicaid into law in 1965 to provide health insurance coverage to low-income Americans through a partnership between states and the federal government. Georgia’s Medicaid program provides almost 2 million Georgians with access to health care. Children make up about 1.3 million Medicaid enrollees, or 66 percent. Another 25 percent of enrollees are seniors, blind or disabled. The remaining 8 percent are low-income pregnant women, parents or Georgians receiving breast and cervical cancer treatment. Low-income adults without dependent children are not eligible for Medicaid because Georgia did not expand Medicaid eligibility under the Affordable Care Act.
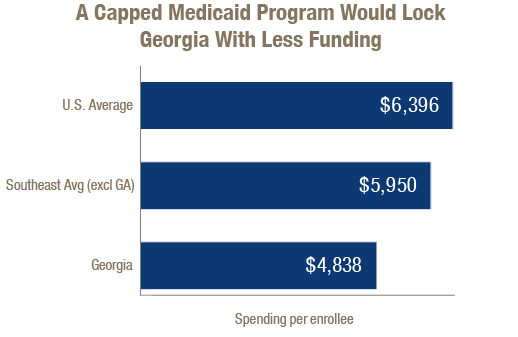
Georgia relies on federal dollars to deliver critical health coverage to vulnerable Georgians. Georgia receives $2.17 in federal matching funds for each $1 the state invests in Medicaid. The state-federal matching structure allows Georgia to draw down more money when there is an economic downturn or higher than expected health care costs. The AHCA restructures this to a per-capita cap system, which is a fixed payment to the state for each enrollee. The fixed payment would be based on historical costs for each eligibility category, such as child, non-elderly adult, elderly and disabled. Georgia consistently ranks as one of the lowest spending states for Medicaid. Georgia is the 45th ranked state in Medicaid spending per enrollee and a capped system cements that low status.[4]
 Georgia stands to receive less money than other states per Medicaid enrollee in the AHCA, leaving very little to no room for painless cuts. Georgia already runs a lean and efficient Medicaid operation, spending less on administrative costs than private insurance companies and controlling per enrollee spending growth. Most Georgia Medicaid enrollees are covered by a managed care plan. These plans reduced per enrollee costs per member by 1.7 percent from 2009 to 2015.[5]
Georgia stands to receive less money than other states per Medicaid enrollee in the AHCA, leaving very little to no room for painless cuts. Georgia already runs a lean and efficient Medicaid operation, spending less on administrative costs than private insurance companies and controlling per enrollee spending growth. Most Georgia Medicaid enrollees are covered by a managed care plan. These plans reduced per enrollee costs per member by 1.7 percent from 2009 to 2015.[5]
Georgia is expected to lose $4 billion in federal funding over 10 years under the proposed per-capita cap.[6] If that happens, Georgia budget writers could find the money through cuts to Medicaid eligibility, benefits or health care provider payments. Or the state could increase its spending by 8 percent, putting a strain on Georgia’s budget and taking money away from other state priorities such as education, public safety and transportation. Medicaid cuts will directly impact the health coverage of Georgia’s children, veterans, seniors and people with disabilities. Additional funding for substance abuse treatment services are also at risk under the proposed Medicaid changes.
Medicaid a Critical Support for Georgia Veterans
Medicaid provides health coverage to 50,000 Georgia veterans, allowing them to get the health services they need. Some veterans do not meet requirements for health insurance through the Department of Veterans Affairs (VA) because they lack minimum service time or qualifying disability and discharge status. And for many rural veterans who do not live near a qualified health care provider, it is very difficult to use these services. Veterans are more likely to have complex health care issues that result from their service. These could include traumatic brain injuries or post-traumatic stress disorder. Medicaid helps cover the higher costs of some of these services so veterans get the treatment they need with little or no out of pocket expense.
On top of capping Medicaid spending, the AHCA ends the enhanced funding for eligibility expansion in 2020. The 2010 health law allows states to receive 100 percent federal funding for three years to expand Medicaid eligibility, gradually dropping to 90 percent in 2020 and beyond. States that expanded Medicaid eligibility to low-income adults experienced a large increase in coverage and use of substance abuse treatment services.[7] Georgia did not expand Medicaid and if the expansion opportunity ends, the state loses the opportunity to extend health coverage to 159,000 uninsured Georgians with a mental illness or substance abuse disorder.[8]
Federal Health Care Bill Poses Big Financial Risk for Georgia Hospitals
Georgia hospitals receive nearly $9.5 billion in Medicaid payments, or about 12 percent of combined revenue.[9] Medicaid is a major source of payment for key health services in Georgia, including more than half of all the state’s births. Medicaid is also the primary payer for 75 percent of Georgia’s nursing home patients. The proposed cuts to Medicaid shrink Georgia’s federal Medicaid funding by 4.2 percent over 10 years.[10] This translates to a loss of $3.4 billion over 10 years to Georgia’s hospitals.[11] A loss of Medicaid funding jeopardizes the financial sustainability of hospitals, leaving them with more bad debt as they treat more patients with fewer benefits or no coverage. Half of Georgia’s children are covered by Medicaid, so children’s hospitals stand to take the hardest hit from a reduction in Medicaid funding. Hospitals that specialize in mental health services are also at risk because several of them are more dependent than most on Medicaid revenue.
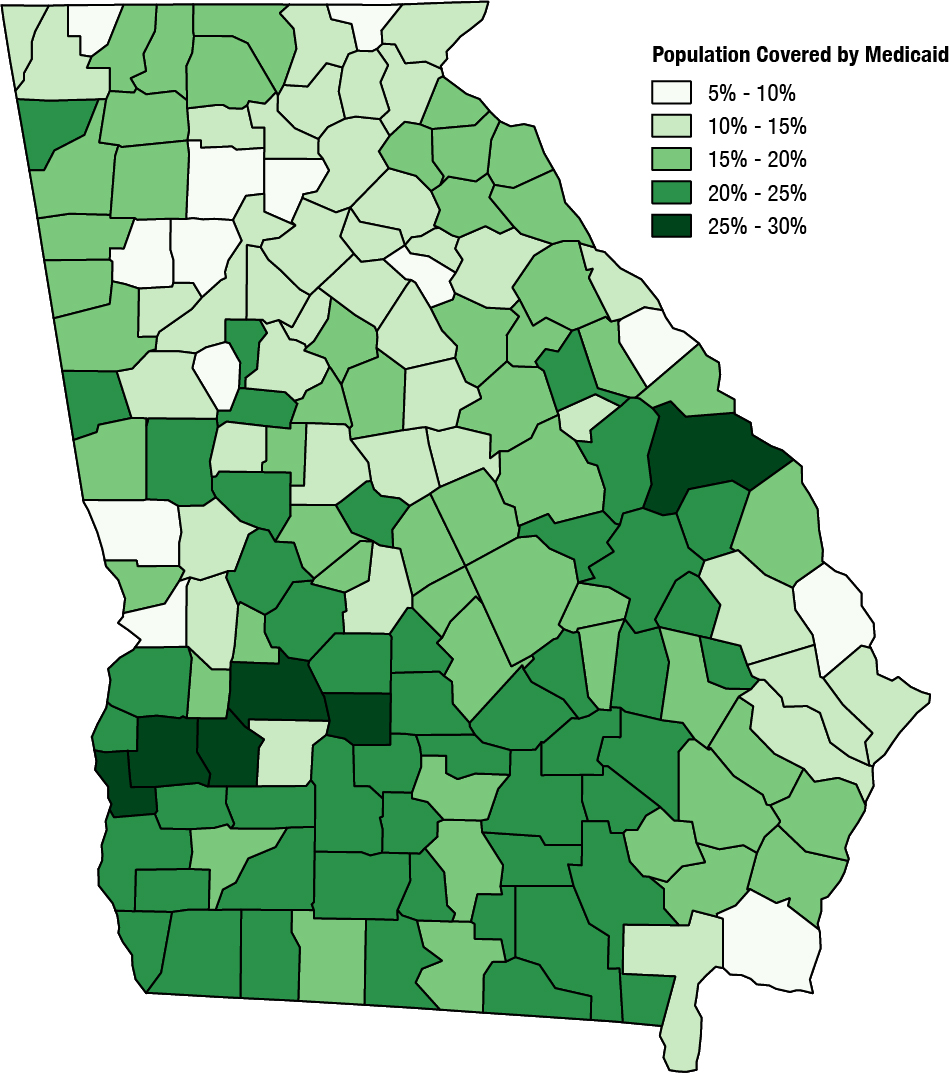
Hospitals in Regions across Georgia Stand to Lose Money in Proposed Health Bill
Medicaid is an important revenue source for both rural and urban hospitals. Rural hospitals get a higher share of their revenue from Medicaid. Hospitals in non-rural counties got an average of 11.5 percent of revenue from Medicaid, while hospitals in rural counties got 13.3 percent of revenue from Medicaid. Six rural hospitals in Georgia closed since 2013 and several others are struggling to keep their doors open. Georgia’s rural counties tend to be home to a higher percentage of Medicaid enrollees because residents there often earn lower average incomes (see Appendix A). Fifty-three percent of children in non-metropolitan areas of Georgia receive Medicaid coverage compared to 39 percent in metropolitan areas.[12] Medicaid covers additional services such as non-emergency medical transportation, which is especially important for rural residents who lack transportation, or need to travel longer distances for health care. A cut to Medicaid places an even greater financial burden on rural hospitals and reduces health care access for rural residents.
Proposed Changes to Ripple Outside of the Hospital Industry
Nursing Homes and Long-Term Care Services
Georgia’s nursing home facilities lose revenue under the AHCA because a large portion of long-term care is funded by Medicaid. About 90 percent of the nursing home facilities in Georgia report the majority of their patient days are covered by Medicaid.[13] Seventy-five percent of Georgia nursing home patients used Medicaid as their primary payer. Medicaid is also critical in supporting long-term services and support outside of institutional settings, allowing seniors and people with disabilities to live at home in their communities. Georgia’s home and community-based services are an optional Medicaid benefit, putting it a greater risk of cuts. Georgia would lose between 3,000 and 7,000 home health aide and personal care aide jobs if these services are reduced.[14]
School Districts
Georgia school districts received $30 million in federal Medicaid reimbursements in 2015 to support the cost of providing health services for students.[15] This money supports schools in delivering services and supports for special education students. Medicaid also pays for preventive services for all children eligible for benefits and helps schools hire nurses, therapists, speech pathologists and other health care professionals.
Economy
The AHCA is estimated to cost Georgia 16,200 jobs by 2026.[16] Georgia might gain jobs initially, but the magnitude of coverage losses in the long run means the state’s economy will likely shrink. Almost all of these jobs are in the health care industry, but other businesses rely on economic activity the health care sector generates. The gross state product is projected to drop by $1.6 billion and business output to drop by $2.5 billion in 2026 compared to projections under the current federal health law.
Marketplace Subsidy Changes to Hurt Older, Rural Georgians Most
By the time the last insurance marketplace open enrollment period ended Jan. 31, 2017, 494,000 Georgians signed up for a health insurance plan. About 87 percent of these Georgians could pay for coverage because they qualified for advance premium tax credits or cost-sharing reductions. The average monthly premium for Georgians receiving a subsidy was $87 compared to the overall marketplace average premium of $431. These tax credits, or subsidies, are based on income and the cost of premiums in the geographic area. The proposed subsidies in the AHCA are based only on age and many Georgians stand to receive less assistance to maintain coverage.
Older Georgians and rural Georgians are the most at risk from the tax credit changes.[17] Health insurance premiums are often higher in rural areas due to fewer insurers and a smaller pool of enrollees. The AHCA’s proposed tax credit doesn’t adjust based on the higher premiums in high-cost markets. Older low to moderate-income Georgians would also be hurt by the increase in the age rating. Under the AHCA, insurers can charge older people up to five times more than younger people. That compares to three times more under current law.
 Georgians with Pre-Existing Conditions, Costly Health Needs Lose Protections
Georgians with Pre-Existing Conditions, Costly Health Needs Lose Protections

The AHCA gives states the option to define their own essential health benefits standards and to allow insurers to charge higher premiums based on health status. Nearly 1.8 million Georgians or 29 percent of the state’s population carry a pre-existing condition not covered under insurance underwriting practices before the Affordable Care Act.[18] These Georgians will find plans to cover the services they need scarce if essential health benefits standards are repealed. Without these standards, insurance companies can drop coverage for chemotherapy, high-cost drugs, or other costly services people with pre-existing conditions often need.
Under the Affordable Care Act, plans that covered all essential health benefits could not impose annual and lifetime limits. Insurance plans can reinstate annual and lifetime limits in states that change essential health benefits standards. About 3.3 million Georgians are no longer constrained by lifetime limits on their insurance plans because of the Affordable Care Act.
Georgia appears poised to pursue one or both of these options. In a January 2017 letter to the U.S. House of Representatives leadership, Georgia’s insurance commissioner asked for Congress to give states more power to regulate insurance. Securing these state waivers puts millions of Georgians at risk of losing health benefits or being one major illness away from medical bankruptcy.
Public Health Funding Loss Weakens Georgia’s Health Status and Economy
The Affordable Care Act created the Prevention and Public Health Fund as the country’s first mandatory source of money for preventing disease, improving health outcomes and reducing health care costs. The AHCA proposes to eliminate the fund, which is used to give grants to state and local public health departments. Georgia stands to lose $20 million a year in public health funding over five years.[19] This funding is critical for responding to epidemics, preventing chronic disease, and other efforts to improve the health of all Georgians.
This fund provides $890 million to Atlanta’s Centers for Disease Control and Prevention. Cutting this fund would likely impact jobs at the agency because the money makes up 12 percent of its budget. The agency is one of the largest employers in metro Atlanta.
Conclusion
The American Health Care Act threatens the wellbeing of vulnerable Georgians and threatens to significantly reduce funding for Georgia’s health care system. Preserving the structure of Medicaid is critical for Georgia to avoid putting it at a financial disadvantage relative to other states. Capping Medicaid locks Georgia in at a lower spending level and shifts significant costs to the state. With fewer of these dollars flowing into the state, Georgia’s hospitals and nursing homes, schools, the state budget and the economy will be greatly strained. Reducing funding for marketplace subsidies also removes money from the state and risks the health coverage and benefits of nearly 500,000 Georgians. Millions of Georgians with private insurance, including employer-sponsored plans, are also at risk of losing benefits under proposed state leeway to change essential health benefits.
The AHCA is the basis for the health care bill the U.S. Senate is drafting this month. It is important for Senate leaders to not rush through with a bill that would financially disadvantage Georgia and leave many Georgians with more expensive and less comprehensive health coverage.
References
[1] Urban Institute. “The Impact of Per Capita Caps on Federal and State Medicaid Spending.” March 2017.
[2] Families USA. “Defending Health Care in 2017: What Is at Stake for Georgia.” December 2016.
[3] Claxton G, Cox C, Damico A, Levitt L, Pollitz K. “Pre-existing Conditions and Medical Underwriting in the Individual Insurance Market Prior to the ACA.” December 2016.
[4] Rudowitz R, Valentine A, Ubri P, Zur J. “Factors Affecting States’ Ability to Respond to Federal Medicaid Cuts and Caps: Which States Are Most At Risk?” June 2017.
[5] Health Management Associates. “Medicaid Managed Care in Georgia.” June 2017.
[6] Urban Institute. “The Impact of Per Capita Caps on Federal and State Medicaid Spending.” March 2017.
[7] Bailey P. “Building on ACA’s Success Would Help Millions with Substance Use Disorders.” April 2017.
[8] Department of Health and Human Services. “ASPE Issue Brief: Benefits of Medicaid Expansion for Behavioral Health.” March 2016.
[9] GBPI Analysis of Georgia Department of Community Health Annual Hospital Financial Survey, 2015
[10] Urban Institute. “The Impact of Per Capita Caps on Federal and State Medicaid Spending.” March 2017.
[11] GBPI Analysis of Georgia Department of Community Health Annual Hospital Financial Survey (2015) and March 2017 Urban Institute Estimates
[12] Georgetown University Center for Children and Families and the University of North Carolina. “Medicaid in Small Towns and Rural America: A Lifeline for Children, Families, and Communities.” June 2017.
[13] GBPI Analysis of Georgia Department of Community Health Annual Nursing Home Questionnaire 2016
[14] Leading Age and the Center for Consumer Engagement in Health Innovation. “Capping Medicaid: How Per Capita Caps Would Affect Long-Term Services & Supports and Home Care Jobs.” June 2017.
[15] Shubel J. “Medicaid Helps Schools Help Children.” Center on Budget and Policy Priorities, April 2017.
[16] L. Ku, E. Steinmetz, E. Brantley et al., “The American Health Care Act: Economic and Employment Consequences for States.” The Commonwealth Fund, June 2017.
[17] Kaiser Family Foundation. “Premiums and Tax Credits Under the Affordable Care Act vs. the American Health Care Act: Interactive Maps.” April 2017.
[18] Claxton G, Cox C, Damico A, Levitt L, Pollitz K. “Pre-existing Conditions and Medical Underwriting in the Individual Insurance Market Prior to the ACA.” December 2016.
[19] Trust for America’s Health. “Special Analysis: Prevention and Public Health Fund Federal and State Allocations.” January 2017.






