Improving the prevention and treatment of mental health conditions and substance abuse disorders is critical to ensure the well-being of all Georgians. State lawmakers made significant progress in recent years to improve behavioral health treatment for core challenges of mental health and drug addiction. But Georgia still is home to one of the highest uninsured rates and a rapidly rising number of drug overdose deaths, especially in rural areas. Strengthening both behavioral and physical health treatment and better integrating those services is essential to the quality of life of Georgians and to support the kind of healthy and productive workforce that companies and the state’s economy rely on.
About 1.3 million Georgia adults or 17 percent of adults reported a mental illness in the past year.[1] Mental health conditions are often underdiagnosed and undertreated, making the scope of mental illness even broader. Thirty-two percent of Georgia adults reported poor mental health status in 2016.[2] People with mental illness are more likely to engage in substance abuse than people without mental illness.[3] Mental illness and substance abuse can often occur together, but one does not necessarily cause the other. Drug overdose deaths in Georgia increased every year since 2012. From 2012 to 2016 the number of drug overdoses increased by 35 percent. About 69 percent of these deaths in 2016 were related to opioids, including heroin and synthetic drugs such as oxycodone and morphine.[4]
As state leaders examine options to support children’s mental health and fight the opioid epidemic, it is a good time to examine what works and what can be done to prioritize better access to care and prevention:
- Continue the investment in supportive housing and related services. Supportive housing is a successful program designed to provide permanent and affordable housing in combination with services like case management and peer assistance.
- Implement criminal justice reforms to provide better treatment for people with mental illness. Pre-arrest diversion programs and training for first responders are some of the top strategies to emphasize treatment, rather than criminal punishment for non-violent offenses related to mental illness.
- Adequately invest in early intervention and prevention. Drug overdose deaths in Georgia are increasing and are now on par with automobile crash deaths. It is important to intervene early to provide mental health screening and counseling for affected Georgians from childhood through adulthood.
- Expand health insurance coverage and access to care. Increasing health coverage is necessary to ensure provider services are paid and services are more affordable. Telehealth and integration of behavioral health services with primary care are ways to increase health care access in areas with provider shortages.
Georgia Behavioral Health Care Timeline
 Background
Background
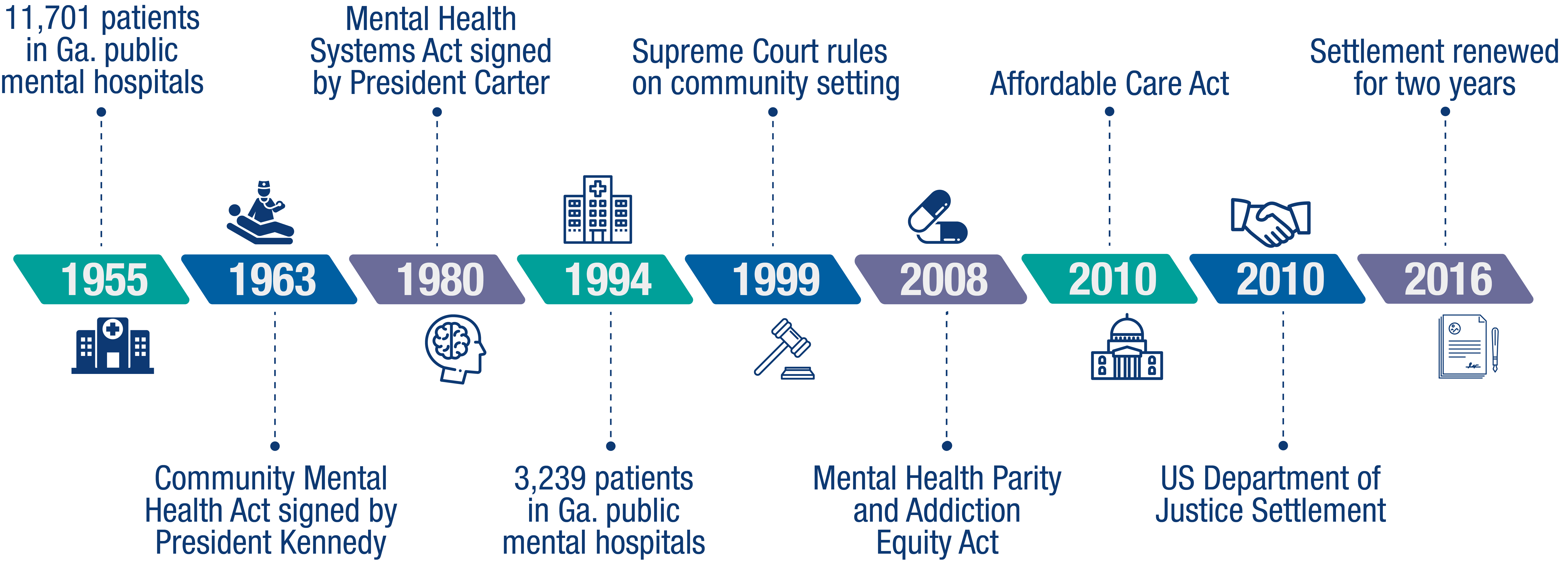
Both mental illness and substance abuse can be treated by behavioral health services such as psychotherapy, counseling or rehabilitation programs. Until the 1960s, many people receiving mental health treatment lived in state psychiatric hospitals. These institutions often drew deserved criticism for poor living conditions. This led to a movement to deliver care in community settings as a way to improve quality of life for patients. The Community Mental Health Act of 1963 funded community mental health centers and played a significant role in deinstitutionalizing mental health care. The Mental Health Systems Act of 1980 continued to support the move away from institutions and it also funded state and local prevention efforts. President Jimmy Carter signed this bill into law, but most of it was repealed by President Ronald Reagan’s administration the following year. Despite the repeal, the shift to community-based mental health care continued. In 1955, 11,701 patients occupied Georgia’s public mental hospitals. That number dropped to 3,239 by 1994.[5]
The U.S. Supreme Court ruled in 1999 that people with developmental disabilities have the right to live in a community setting instead of an institution. Two Georgians with mental illnesses sued the state to secure a transfer from an institution. They remained confined in a psychiatric unit of a state hospital even though an assessment determined they were better suited for community-based treatment. In 2010, the United States Department of Justice and the State of Georgia entered a five-year settlement agreement to transition all people with developmental disabilities from state hospitals to community settings. The settlement agreement is now extended until June 30, 2018.
With more people receiving services in their communities instead of state hospitals, a movement arose to promote mental health parity. Mental health parity means equal treatment of behavioral health conditions and physical health conditions in insurance plan coverage. Behavioral health treatment historically was not covered by insurance plans at the same level as physical health treatment. The Mental Health Parity Act of 1996 prohibited higher annual or lifetime limits for mental health benefits compared to medical benefits. The Mental Health Parity and Addiction Equity Act of 2008 expands on the 1996 law, including substance abuse and prohibiting differences in cost sharing and network coverage for mental health and substance abuse treatment services. The Affordable Care Act of 2010 went further to improve behavioral health coverage by including mental health and substance abuse treatment services in the 10 essential health benefits insurers must offer. These federal laws set the foundation for achieving mental health parity, but challenges remain in fully implementing and enforcing the law.
Support Services Can Help Get People Back on their Feet
States struggle to ensure people get quality housing that supports their treatment once they leave a state hospital. The Georgia Department of Behavioral Health and Developmental Disabilities, along with the Department of Community Affairs, formally agreed in 2015 to provide supported housing. This includes housing vouchers funded by the state and federal governments to provide mentally ill low-income people with affordable housing that is connected to treatment services. Georgia is doing a better job providing supported housing. The initiative placed 3,213 Georgians as of July 1, 2016. However, the settlement goal is to provide 9,000 people with supported housing. The state behavioral health agency also connects people who are underemployed or unemployed due to mental illness with 22 employment support organizations across the state.
 The cost is much higher to deliver behavioral health treatment in an institutional setting than in the community. Supported housing saves the state money by reducing days in a hospital or a nursing home and visits to the emergency room. Providing supportive housing to high-needs groups of homeless individuals with mental illness saves an average of $6,000 a year per person in health care costs, according to one study.[6] States that aim to help the highest need people can reinvest the health care and correctional systems savings into offering more rental assistance.
The cost is much higher to deliver behavioral health treatment in an institutional setting than in the community. Supported housing saves the state money by reducing days in a hospital or a nursing home and visits to the emergency room. Providing supportive housing to high-needs groups of homeless individuals with mental illness saves an average of $6,000 a year per person in health care costs, according to one study.[6] States that aim to help the highest need people can reinvest the health care and correctional systems savings into offering more rental assistance.
Some communities encourage public-private partnerships to provide supported housing. Pine Ridge and Oak Ridge apartments in Rome, Ga. are examples of this model. A private real estate investment corporation developed these apartment buildings with financing from the Georgia Department of Community Affairs. Residents are formerly homeless people with physical or developmental disabilities. The apartment community partners with local behavioral health service providers, such as Highland Rivers Health. This model is not a substitute for adequate government funding for supported housing, but it can help launch new initiatives and demonstrate the savings. Georgia can build on the success of supported housing and employment by examining more ways to reinvest program savings.
Criminal Justice Reform Prioritizes Benefits of Treatment Over Punishment
Treating mental illness and substance abuse is increasingly recognized as a preferred option to sending people to jails or prisons. Georgia lawmakers already made great strides in criminal justice system reforms in recent years, including setting juveniles and nonviolent offenders on the path to rehabilitation rather than prison. But additional policies are needed to prevent the criminalization of people better served with treatment for their health conditions. Some local communities are exploring alternatives to incarceration of people with mental illness and substance abuse problems.
Pre-arrest diversion programs are part of the solution. These programs identify people who are likely to be arrested for a non-violent offense related to substance abuse, like someone caught in possession of a small amount of drugs.[7] Most of these people now wind up with an arrest on their criminal record and are sent to post-arrest programs like a drug court. A pre-arrest diversion program occurs before they are formally charged and places them in treatment services. These programs are proven to reduce recidivism and lower costs to the criminal justice system.[8] People also get more opportunities for employment after treatment, because the diversion program is not part of a criminal record.
Pre-arrest diversion programs are operated by cities and counties, but the state can promote similar work in communities across the state, as well as expand statewide training programs tactics used by police officers and other first responders. Crisis Intervention Training and Mental Health First Aid are offered in Georgia to help officers better understand mental illness and learn how to better respond when confronted with a mental health crisis. The demand for crisis intervention training in Georgia is now greater than availability. Mental Health America of Georgia promotes combining the two kinds of trainings and providing department-wide teaching to continue the success of these programs.[9]
People caught up in the criminal justice system often suffer higher rates of mental illness and substance abuse and need adequate treatment when they are released from jail or prison. One way to support behavioral health treatment adherence for people transitioning out of incarceration is to suspend their Medicaid benefits instead of terminating them. By suspending the benefits, the person will not face any interruptions in their access to health care and this can reduce risk of recidivism.[10] This policy change offers a much broader benefit if the state expanded Medicaid eligibility to low-income adults without affordable coverage options. The income requirements in Georgia are very restrictive for non-elderly adults who do not meet certain requirements such as a breast or cervical cancer diagnosis or pregnancy. For example, a parent in a family of three with children under age 19 can make no more than $6,600 a year.
Early Intervention Helps Prevent Behavioral Health Problems on the Front-End
Drug overdose deaths are increasing in Georgia and are now on par with automobile crash deaths. The growing prevalence of substance abuse disorders and related deaths requires more intervention strategies before people develop dependency on drugs and become at risk of overdose. Deaths by suicide are also increasing in Georgia. Ninety percent of people in the state who die by suicide experience mental illness, according to estimates.[11]
Suicide deaths in Georgia increased 25 percent from 2012 to 2016. The rate of suicide death is much higher in rural Georgia. The suicide rate in rural Georgia counties was 16.8 percent in 2016 compared to 12.9 percent in non-rural counties.[12]
Rate of Suicide Death Higher in Rural Georgia, Targeted Early Intervention Needed

Georgia lawmakers passed the Jason Flatt Act in 2015 to require suicide prevention education training for some public school workers. Interventions in a school-based setting can be effective in early detection and treatment of mental illness and substance abuse. The state behavioral health agency piloted the Georgia Apex Program in 2015 to provide school-based mental health services. In the first year, 2,400 students were referred for the first time to behavioral health services. About 85 percent of services were billed to Medicaid and PeachCare for Kids. These programs provide critical funding for mental health treatment in Georgia. In 2017, the state increased funding to cover mental health services for children from birth to age five. Gov. Nathan Deal also formed a Commission on Children’s Mental Health in June 2017 to recommend ways to improve mental health services for children.
Of the school-aged children across the country who get mental health services, about 80 percent receive them at school through nurses, counselors, phycologists and social workers.[13] Another school-based strategy for behavioral health is known as Screening, Brief Intervention and Referral to Treatment. Substance abuse often starts at a young age, with 90 percent of adult Americans with a disorder reporting smoking, drinking or using other drugs before they turned 18.[14] Until 2017, Georgia was one of only 12 states that did not reimburse schools for these services through Medicaid. The recent change to reimburse for these services can help prevent substance abuse problems at a young age.
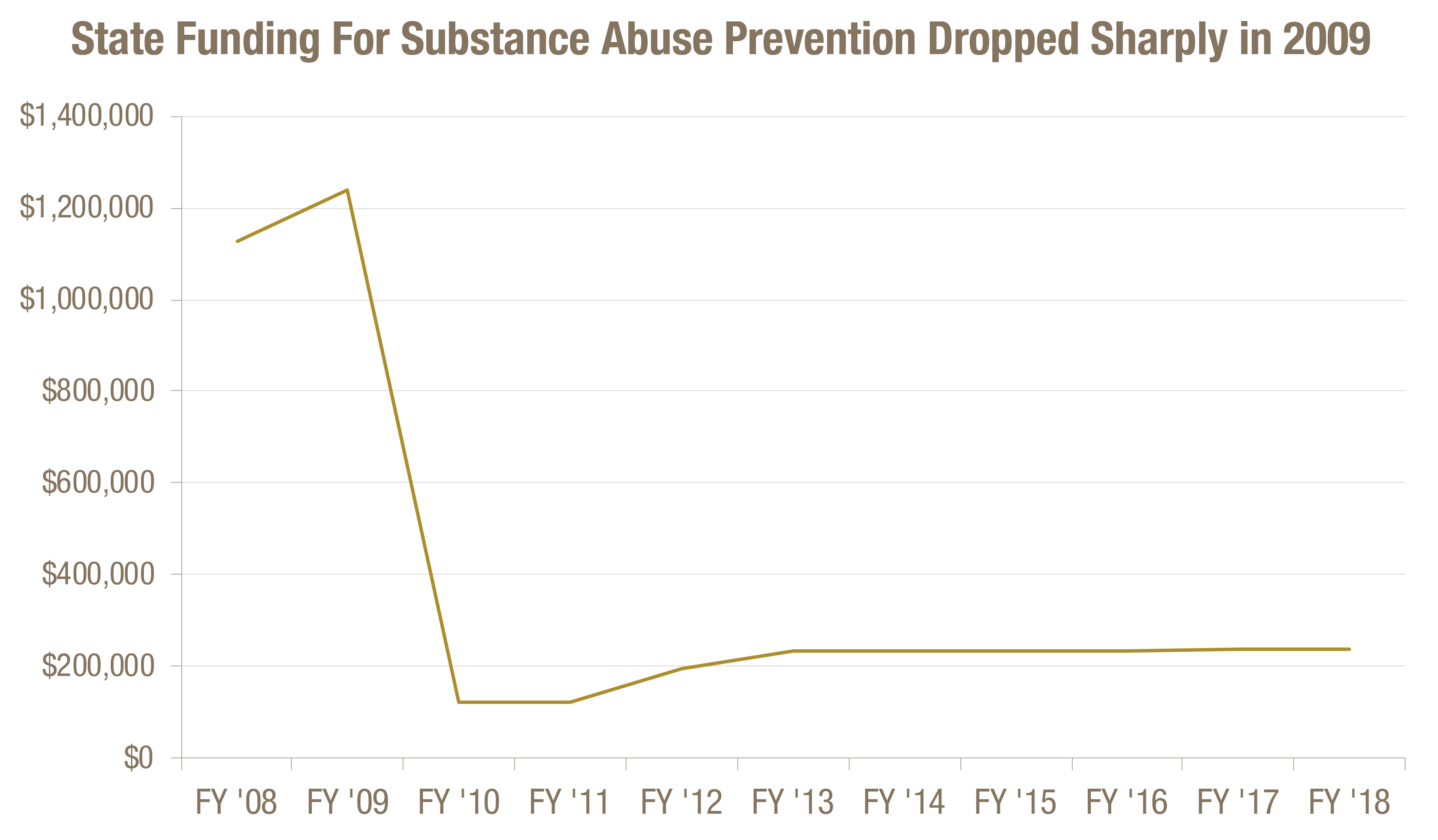
Early intervention services for children and adolescents are getting better, but the need remains to reverse recession-era funding cuts for substance abuse prevention. The state invested $1.1 million for prevention programs aimed at reducing substance abuse in 2008 and $1.2 million in 2009. The state cut funding for prevention efforts to $121,627 in 2010, as it slashed the overall budget. An increase in federal funding from $10.2 million to $22.9 million from 2008 to 2009 helped to offset some of lost state dollars. Federal funding for the effort decreased since then to about $10 million. The state has yet to offset the drop in federal funding, even as the need continues to grow.
 Georgia and other states are taking steps to prevent over-prescription of opioids through drug monitoring programs. Georgia established the Prescription Drug Monitoring Program in 2009, but only about 10 percent of prescribers in the state register. Participation was encouraged but no one was required to check the system before prescribing. The Georgia General Assembly passed a measure to require everyone who writes prescriptions to register in the program by January 2018. Starting July 2018, prescribers will be required to check the system before prescribing opiates.[15] These changes are designed to help the state reduce over-prescription of opioids. About half of prescription writers registered for the program by fall 2017. The state can help prescribers more quickly adopt the new program by integrating the resulting data into electronic health records and health information exchanges.[16]
Georgia and other states are taking steps to prevent over-prescription of opioids through drug monitoring programs. Georgia established the Prescription Drug Monitoring Program in 2009, but only about 10 percent of prescribers in the state register. Participation was encouraged but no one was required to check the system before prescribing. The Georgia General Assembly passed a measure to require everyone who writes prescriptions to register in the program by January 2018. Starting July 2018, prescribers will be required to check the system before prescribing opiates.[15] These changes are designed to help the state reduce over-prescription of opioids. About half of prescription writers registered for the program by fall 2017. The state can help prescribers more quickly adopt the new program by integrating the resulting data into electronic health records and health information exchanges.[16]
Targeted Behavioral Health Solutions Most Crucial in Rural Georgia
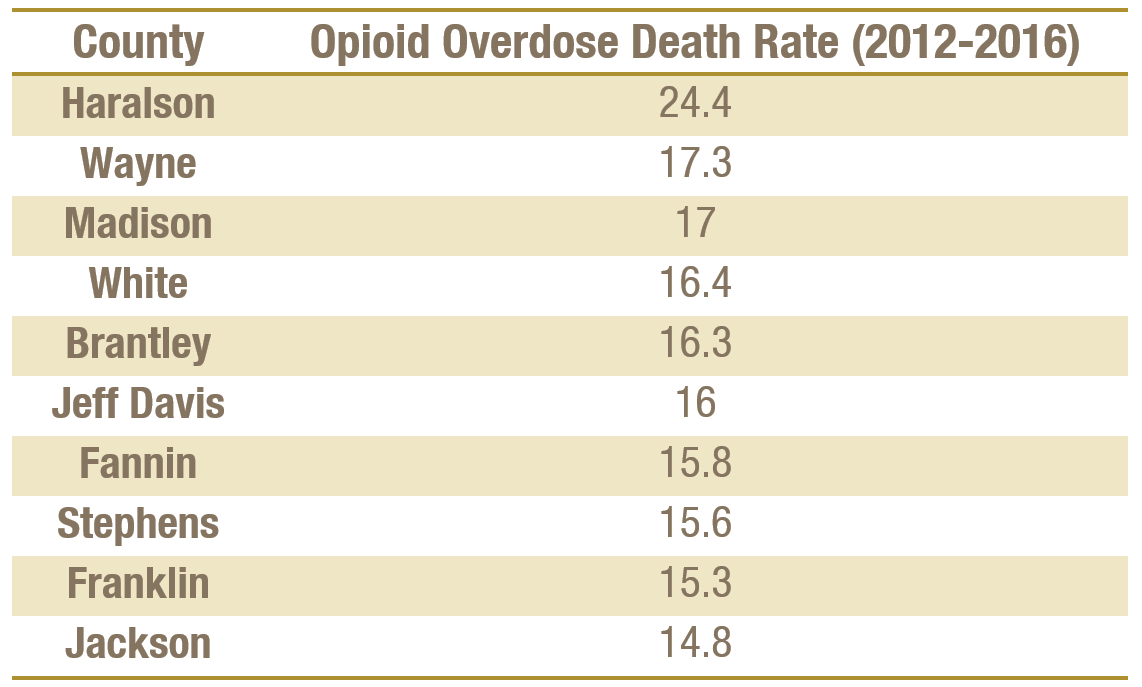
The rising rate of drug overdose deaths is most acute in rural Georgia. Drug overdose deaths increased 35 percent statewide from 2012 to 2016. The majority are opioid-related. Sixty percent of the 55 Georgia counties with drug overdose deaths above the national average are rural areas with limited substance abuse treatment.[17] The chart below shows the 10 Georgia counties with the highest opioid overdose death rates from 2012 to 2016.
Rural Georgia Counties Suffer Highest Opioid Overdose Death Rates[18]
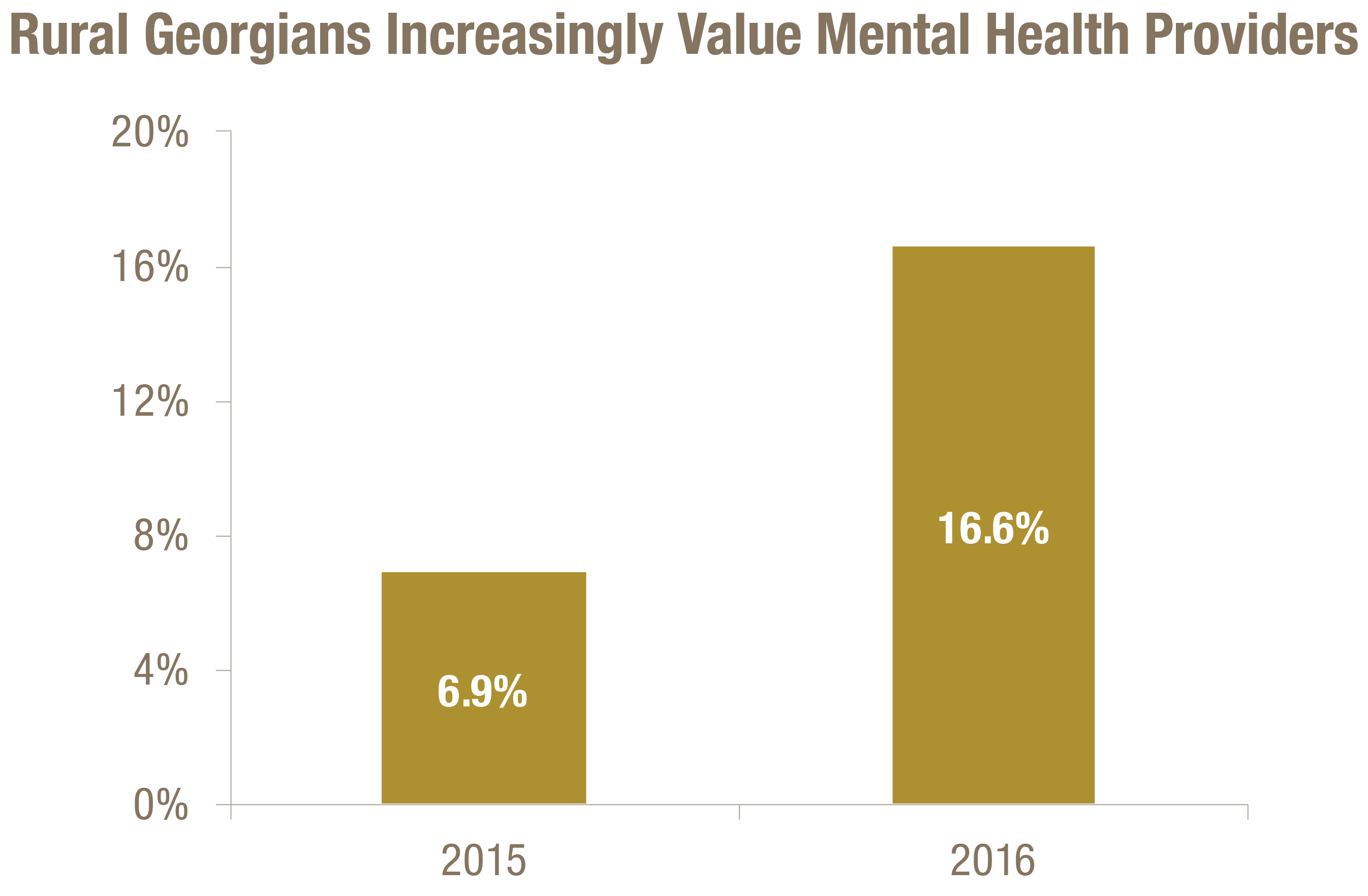
Access to care for all types of health care services is a continuing challenge in rural Georgia. Ninety-eight of Georgia’s 108 rural counties are short on mental health professionals.[19] Rural Georgians are increasingly concerned about a scarcity of mental health providers. A 2015 survey of more than 1,900 rural Georgians found 6.9 percent said mental health professionals delivered the greatest impact on the health of the community. That percentage rose to 16.6 in 2016.[20]
Increasing the capacity of behavioral health providers across the state requires continued efforts to support professionals through scholarships and loan repayment as well as expanded scope of practice.[21] One effective way to increase provider capacity in underserved rural areas is to support pipeline training programs for rural residents and build a more diverse, culturally competent workforce.[22] Another way to support access to care is to increase the number of support professionals, including community health workers and peer specialists. Georgia is a leader in this work through its peer support services. Peer support specialists have lived with mental health, trauma or substance abuse. They are trained and certified to support their peers during treatment and recovery. Georgia became the first state to provide Medicaid reimbursement for peer specialists in 1999.[23] The state can build on this success by enhancing a pipeline for these specialists to train for careers as mental health counselors or psychiatrists.
Increased access to care in rural areas can also get a boost through integration of care to holistically treat a patient’s needs. This is especially true for rural communities that often face poorer health status and more access barriers. Rural counties are also more likely to be home to a primary care provider than a mental health specialist. So it is important for the primary care provider to incorporate behavioral health screenings and referrals. Some communities integrate medical care and behavioral health care, as well as dental care and home health services. One, called the social-medical model, is proving effective in treating the health of patients with complex needs.[24] This model integrates care and also provides supports to solve problems like a lack of transportation, housing and healthy food. Georgia can incorporate these models through Medicaid for patients with multiple chronic conditions.
Transportation poses a significant barrier in much of rural Georgia, often requiring a long trip to get services. The state operates a telehealth network to lessen this barrier and allow residents to make appointments with providers using digital connections across the state. Private insurers must cover payment for telehealth services on par with what is offered for the same in-person service for it to work. Private insurers that don’t already offer in-person behavioral health services are not required to do so under parity laws. Medicaid covers telehealth services and is one of the main payers of these services, especially in school-based telehealth programs.[25] Telemedicine is a promising strategy for improving access to behavioral health care, but a remaining challenge is broadband access and extending coverage so that there is payment for these services. In a study of 12,000 rural Georgians, 16 percent responded, “I can’t get wireline service.” Although telehealth sites are available in all 159 Georgia counties, there is a need for increased broadband for more residents to receive telehealth services at home.
Georgia Can Expand Health Coverage to Help Pay for Behavioral Health Treatment
The Affordable Care Act of 2010 aimed to increase health coverage through the creation of health insurance marketplaces for individual plans and the expansion of the Medicaid program to cover more low-income residents. Under the federal health law, Georgia’s uninsured rate dropped 27 percent from 2010 to 2015.[26] However, the need remains for better access to behavioral health care in Georgia. Thirteen percent of Georgians lack health insurance and 5 million Georgians live in one of the state’s 103 federally designated mental health professional shortage areas.[27] Most of these shortage areas are in rural counties.

Georgia lawmakers declined Medicaid expansion, which would cover more than 300,000 Georgians who make too much to qualify under the state’s current Medicaid rules and too little to receive tax credits in the health insurance marketplace. That leaves a coverage gap. About 25 percent of uninsured low-income Georgians who would qualify for Medicaid expansion coverage suffer from mental illness or substance abuse.[28] This presents an opportunity to increase access to behavioral health services and a funding mechanism to deliver these services to more Georgians.
States that expanded Medicaid enjoyed success in connecting more people with mental illness or substance abuse disorder with treatment services. Kentucky experienced an increase of 700 percent in Medicaid beneficiaries using substance use treatment services after the state expanded income eligibility in 2014. Medicaid expansion also helped significantly increase coverage for states battling the opioid epidemic. West Virginia suffered the highest drug overdose death rate in 2015. In 2013, 23 percent of substance use and mental health disorder hospitalizations were uninsured West Virginians. This share dropped to 5 percent at the end of 2014.[29]
Expanding Medicaid will also help pay for successful strategies such as providing housing with support services. Through the Medicaid program, states get the flexibility to cover services such as case management and personal care. States can also work with Medicaid managed care organizations to coordinate supportive housing services.
Georgia can also leverage the Medicaid program to increase behavioral health services by pursuing federal waivers. States can apply for so-called Section 1115 waivers to test new Medicaid policies and delivery approaches. Several states are using these waivers to expand their Medicaid program using innovative approaches, such as paying for private insurance instead of covering residents through the state’s managed care plans. The federal Medicaid agency issued new guidance this year for states to receive federal funds for a continuum of services to treat addiction to opioids and other substances. State would now be eligible to receive federal funds for Medicaid enrollees living in residential treatment facilities.[30] This is an option Georgia can consider, but it will be most effective if the waiver also closes the coverage gap.
Conclusion
Georgia is making progress to strengthen behavioral health treatment through initiatives such as supported housing and employment, improvements to the prescription drug monitoring program and offering law enforcement training to make the criminal justice system work better for people with mental illness and substance abuse disorders.
But much is left to do to increase health coverage, improve access to behavioral health care in rural areas and reduce deaths due to the growing opioid epidemic across the state. Georgia can build on its progress by making it a top priority to increase funding for substance abuse prevention, integrate behavioral health care with primary care services and expand access to care for Georgians without health coverage.
Endnotes
[1] “Adults Reporting Mental Illness in the Past Year.” The Kaiser Family Foundation State Health Facts. Data Source: Substance Abuse and Mental Health Services Administration (SAMHSA), Center for Behavioral Health Statistics and Quality, National Survey on Drug Use and Health (NSDUH), 2014 and 2015.Endnotes
[2] “Percent of Adults Reporting Poor Mental Health Status.” The Kaiser Family Foundation State Health Facts. Data Source: Kaiser Family Foundation analysis of the Centers for Disease Control and Prevention (CDC)’s Behavioral Risk Factor Surveillance System (BRFSS) 2013-2016 Survey Results.
[3] “Co-occurring Disorders.” Substance Abuse and Mental Health Services Administration. March 2016.
[4] Online Analytical Statistical Information System. Georgia Department of Public Health, Office of Health Indicators for Planning.
[5] “Deinstitutionalization: A Psychiatric ‘Titanic’.” FRONTLINE. May 2005. An excerpt from Out of the Shadows: Confronting America’s Mental Illness Crisis by E. Fuller Torrey, M.D.
[6] Dohler E, Bailey P, Rice D, Katch H.“Supportive Housing Helps Vulnerable People Live and Thrive in the Community.” Center on Budget and Policy Priorities. May 2016.
[7] Carlos R. Martinez. “Community Alternatives to Arrest for Problematic Alcohol and Drug Use.” Community Catalyst. September 2017.
[8] “No Entry: A National Survey of Criminal Justice Diversion Programs and Initiatives.” The Center for Health and Justice at TASC. December 2013.
[9] 2017 Legislative Priorities. Mental Health America of Georgia.
[10] Judith Solomon. “Medicaid Can Support Transitions Back to the Community.” Center on Budget and Policy Priorities. April 2016.
[11] “Suicide: 2016 Facts and Figures.” American Foundation for Suicide Prevention.
[12] Online Analytical Statistical Information System. Georgia Department of Public Health, Office of Health Indicators for Planning.
[13] “Final Report of the House Study Committee on Children’s Mental Health.” Georgia House of Representatives Children’s Mental Health Study Committee. December 2015.
[14] “SBIRT – A Preventative Approach to Address Youth Substance Abuse.” Presentation by Georgia Council on Substance Abuse to the Georgia House Study Committee on Children’s Mental Health. November 2015.
[15] “Prescription Drug Monitoring Program.” Georgia Department of Public Health. August 2017.
[16] “Integrating & Expanding Prescription Drug Monitoring Program Data: Lessons from Nine States.” Division of Unintentional Injury Prevention, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. February 2017.
[17] “Prescription Opioids and Heroin Epidemic in Georgia.” Substance Abuse Research Alliance, Georgia Prevention Project. 2017.
[18] Online Analytical Statistical Information System. Georgia Department of Public Health, Office of Health Indicators for Planning.
[19] Gary D. Nelson. “The two Georgias: Disparities in rural health and healthcare.” Journal of the Georgia Public Health Association. Vol. 5, No. 4.
[20] HealthVoices: Rural Health and Healthcare: 2016 Georgia Survey Results, Conducted by Matthew Towery, Opinion Savvy LLC, and Reported by Healthcare Georgia Foundation, Issue 3, Publication #100, February 2017.
[21] Tim Sweeney.“Prescribing Remedies for Georgia’s Medical Provider Shortage.” Georgia Budget and Policy Institute. June 2016.
[22] Laura Harker. “Unlocking the Benefits of an Inclusive Health Workforce.” Georgia Budget and Policy Institute. October 2016.
[23] Clayton Velicer. “Georgia Provides a Model for Medicaid Reimbursement of Peer Support Specialists.” Peers for Progress. October 2013.
[24] “Improving Healthcare Value in Rural America.” Healthcare Value Hub. October 2017.
[25] “50-State Survey of Telemental/Telebehavioral Health” Epstein Becker Green. 2016.
[26] Garrett B and Gangopadhyaya A. “Who Gained Health Insurance Coverage Under the ACA, and Where Do They Live?” Urban Institute. December 2016.
[27] “Mental Health Care Health Professional Shortage Areas (HPSAs).” The Kaiser Family Foundation State Health Facts. Data Source: Bureau of Health Workforce, Health Resources and Services Administration (HRSA), U.S. Department of Health & Human Services, Designated Health Professional Shortage Areas Statistics: Designated HPSA Quarterly Summary, as of December 31, 2016.
[28] Dey J, Rosenoff E, West K. “Benefits of Medicaid Expansion for Behavioral Health.” U.S. Department of Health and Human Services, Assistant Secretary for Planning and Evaluation. March 2016.
[29] “Continuing Progress on the Opioid Epidemic: The Role of the Affordable Care Act.” U.S. Department of Health and Human Services, Assistant Secretary for Planning and Evaluation. January 2017.
[30] “Re: New Service Delivery Opportunities for Individuals with a Substance Use Disorder.” Center for Medicare and Medicaid Services Letter to State Medicaid Directors.






